
TUBERCULOSIS INTESTINAL (TI)
Es una patología inflamatoria infecciosa ocasionada por Mycobacterium tuberculosis. La TI constituye la forma más frecuente de presentación extrapulmonar, coexistiendo con la afección pulmonar en alrededor del 25% de casos.
1.
Endoscopía
1.1
Localización: Puede comprometer todo el tracto digestivo; sin embargo, la mayor afección se localiza en la región ileocecal probablemente por la mayor estasis fisiológica y la presencia de tejido linfoide.
1.2
Aspecto:
- Afectación segmentaria con presentación variable
- Nodularidad de la mucosa
- Tumoraciones
- Erosiones y úlceras (circunferenciales o transversales)
- Pliegues deformados
- Estenosis
- Pólipos
- Válvula ileocecal distendida y deformada
2.
Microscopía
2.1
Arquitectura:
- Vellosidades y criptas variables (desde normales hasta atróficas/distorsionadas)
- Úlceras usualmente no penetran más allá de la muscularis mucosae
2.2
Epitelio:
- Cambios regenerativos (aspecto basófilo)
- Reducción de citoplasma y pérdida de mucina
2.3
Infiltrado inflamatorio:
- Linfocitos y células plasmáticas
- Neutrófilos y eosinófilos pueden estar presentes
- Granulomas característicos (>400μm, coalescentes, profundos)
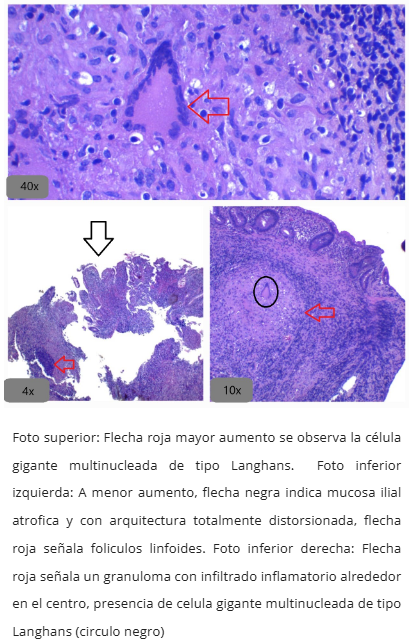
- Necrosis caseosa y células gigantes tipo Langhans frecuentes
- Folículos linfoides en interfaz mucosa-submucosa
- Linfocitos intraepiteliales generalmente normales
3.
Estudios complementarios
3.1
Ziehl Neelsen: Identifica bacilos ácido-alcohol resistentes (rojos en fondo celeste)
3.2
GMS (plata metanamina de Gomori): Puede resaltar bacilos de M. tuberculosis
3.3
Inmunohistoquímica para tuberculosis: Detecta antígenos como estructuras granulares gruesas
3.4
CD73: Marcador útil para distinguir de Crohn (positivo en TB, negativo en Crohn)
4.
Criterios para el diagnóstico
El gold standard diagnóstico es microbiológico, pero el estudio histológico es usado regularmente como apoyo diagnóstico. Se requiere:
- Identificación de características microscópicas mencionadas (granulomas son altamente sugerentes pero no siempre presentes)
- Estudio complementario positivo (Ziehl Neelsen, IHQ o PCR en tejido)
5.
Diagnóstico diferencial histológico
5.1
Enfermedad de Crohn (EC):
- Similitudes: localización ileocecal, alteración arquitectural, inflamación basal
- Diferencias: EC muestra más frecuentemente compromiso ano-rectal, úlceras longitudinales/aftosas y apariencia en "empedrado"
- CD73 negativo en Crohn, positivo en TB
6.
Referencias
- Ihama Y, Hokama A, Hibiya K, Kishimoto K, Nakamoto M, Hirata T, Kinjo N, Cash HL, Higa F, Tateyama M, Kinjo F, Fujita J. Diagnosis of intestinal tuberculosis using a monoclonal antibody to Mycobacterium tuberculosis. World J. Gastroenterol. 2012 Dec 21;18(47):6974-80.
- Al-Zanbagi AB, Shariff MK. Gastrointestinal tuberculosis: A systematic review of epidemiology, presentation, diagnosis and treatment. Saudi Journal of Gastroenterology 2021;27(5):261-274.
- Al Karawi MA, Mohamed AE, Yasawy MI, et al. Protean manifestation of gastrointestinal tuberculosis: report on 130 patients. J Clin Gastroenterol. 1995;20(3):225-232.
- Mukewar S, Mukewar S, Ravi R, Prasad A, Dua KS. Colon tuberculosis:endoscopic features and prospective endoscopic follow-up after anti-tuberculosis treatment. Clin Transl Gastroenterol. 2012;3(10):e24.
- Chatzicostas C, Koutroubakis IE, Tzardi M, Roussomoustakaki M, Prassopoulos P, Kouroumalis EA. Colonic tuberculosis mimicking Crohn's disease: case report. BMC Gastroenterol. 2002;2:10.
- Naga MI, Okasha HH, Ismail Z, El-Fatatry M, Hassan S, Monir BE. Endoscopic diagnosis of colonic tuberculosis. Gastrointest Endosc. 2001;53(7):789-793.
- Sato S, Yao K, Yao T, et al. Colonoscopy in the diagnosis of intestinal tuberculosis in asymptomatic patients. Gastrointest Endosc. 2004;59(3):362-368.
- Pulimood AB, Ramakrishna BS, Kurian G, Peter S, Patra S, Mathan VI, Mathan MM. Endoscopic mucosal biopsies are useful in distinguishing granulomatous colitis due to Crohn's disease from tuberculosis. Gut. 1999;45(4):537-41.
- Khor TS, Fujita H, Nagata K, Shimizu M, Lauwers GY. Biopsy interpretation of colonic biopsies when inflammatory bowel disease is excluded. J Gastroenterol. 2012;47:226-248.
- Lamps LW. Infective disorders of the gastrointestinal tract. Histopathology. 2007;50(1):55-63.
- Cheng W, Zhang S, Li Y, Wang J, Li J. Intestinal tuberculosis: clinico-pathological profile and the importance of a high degree of suspicion. Trop Med Int Health. 2019;24(1):81-90.
- Karimi S, Shamaei M, Pourabdollah M, et al. Histopathological findings in immunohistological staining of the granulomatous tissue reaction associated with tuberculosis. Tuberc Res Treat. 2014;2014:858396.
- Tandon HD, Prakash A. Pathology of intestinal tuberculosis and its distinction from Crohn´s disease. Gut, 1972,13,260-269.
- Brees DJ, Reimer SB, Cheville NF, Florance A, Thoen CO. Immunohistochemical detection of Mycobacterium paratuberculosis in formalin-fixed, paraffin-embedded bovine tissue sections. J Vet Diagn Invest. 2000;12(1):60-63.
- Watermeyer GA, Locketz M. CD73 expression in tissue granulomas in distinguishing intestinal tuberculosis from Crohn's disease in a South African cohort. Scand J Gastroenterol. 2018;53(10-11):1217-1221.
- Odze RD, Goldblum JR: Surgical Pathology of the GI Tract, Liver, Biliary Tract, and Pancreas, 2nd ed. Elsevier: Philadelfia 2009.
Imágenes
Tuberculosis intestinal - Hallazgos endoscópicos
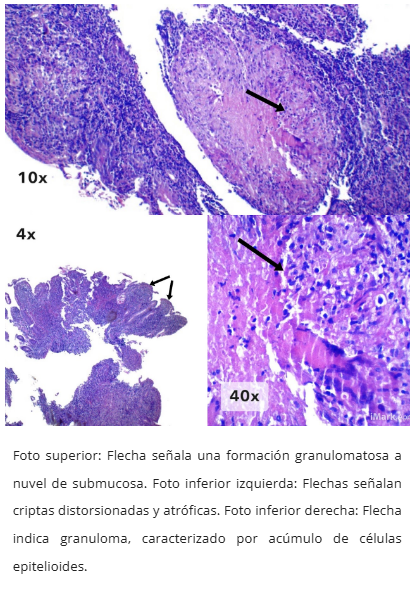
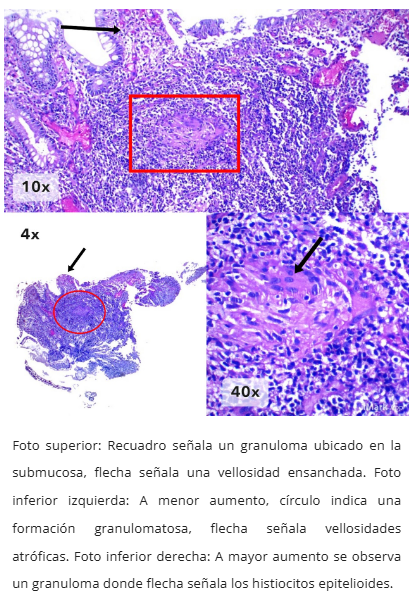
Granulomas tuberculosos característicos
Microscopía de tuberculosis intestinal
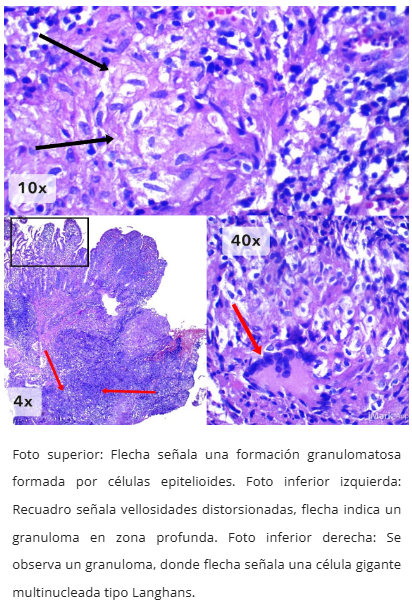
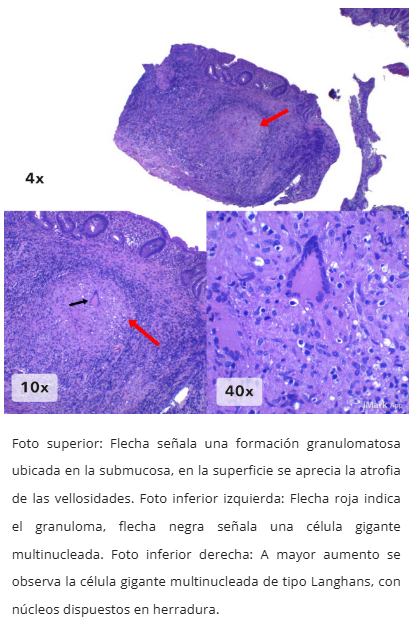
Células gigantes tipo Langhans
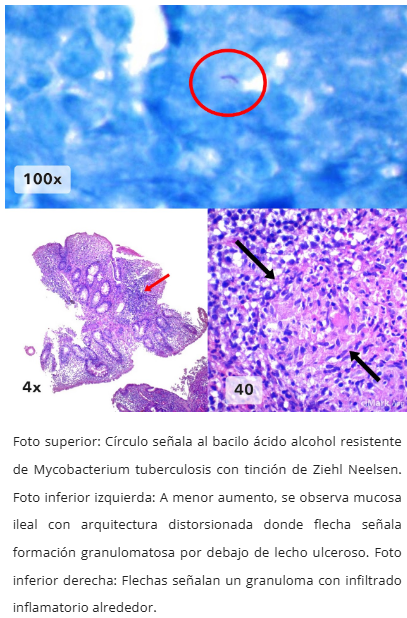
Tinción Ziehl Neelsen para bacilos ácido-alcohol resistentes
Inmunohistoquímica para tuberculosis
