
ADENOCARCINOMA HEPATOIDE DE ESTÓMAGO
Carcinoma poco frecuente y poco reconocido de etiología poco clara, que se caracteriza principalmente por semejar un carcinoma hepatocelular al estudio microscópico. También conocido como HAS (Hepatoid Adenocarcinoma of the Stomach).
1.
Endoscopía:
1.1
Localización: Más común en antro gástrico
1.2
Aspecto: Generalmente se presenta como Bormann tipo III (ulcero-infiltrante)
2.
Microscopía:
2.1
Arquitectura:
- Patrón de crecimiento en nidos o trabéculas similar a carcinoma hepatocelular
- Frecuentemente asociado a componente glandular convencional
2.2
Población neoplásica:
- Células grandes con citoplasma eosinofílico
- Núcleos pleomórficos con cromatina grumosa
- Nucléolos prominentes
3.
Estudio complementario de inmunohistoquímica:
3.1
Positivos:
- AFP (>50% casos) - patrón de membrana o citoplasmático granular
- Glypican 3 (expresión difusa) - membrana o citoplasma
- SALL4 (nuclear) - marcador de células germinales
3.2
Negativos:
- HepPar 1 (usualmente negativo)
4.
Criterios diagnósticos: Requiere:
4.1
Patrón histológico trabecular o en nidos similar a HCC
4.2
Confirmación con inmunohistoquímica (AFP, Glypican 3)
5.
Gradación histológica: No existe sistema estandarizado.
6.
Tipificación histológica: Actualmente no disponible por limitados estudios.
7.
Estadiaje: Según sistema AJCC para adenocarcinoma gástrico.
8.
Diagnóstico diferencial:
8.1
Carcinoma hepatocelular metastásico:
- CK20/CK19 frecuentemente positivos en HAS (negativos en 90% HCC)
- HepPar 1 usualmente negativo en HAS (positivo en HCC)
- Contexto clínico fundamental (metástasis gástrica de HCC es muy rara)
9.
Referencias:
- WHO Classification of Tumours, Digestive System Tumours. 5th edition, volume 1. 2019.
- Xia R, Zhou Y, Wang Y, Yuan J, Ma X. Hepatoid Adenocarcinoma of the Stomach: Current Perspectives and New Developments. Front Oncol. 2021;11:633916.
- Zeng XY, Yin YP, Xiao H, et al. Clinicopathological Characteristics and Prognosis of Hepatoid Adenocarcinoma of the Stomach. Curr Med Sci. 2018;38(6):1054-1061.
- Wang Y, Sun L, Li Z, et al. Hepatoid adenocarcinoma of the stomach: a unique subgroup with distinct clinicopathological and molecular features. Gastric Cancer. 2019;22(6):1183-1192.
- Zhang ZR, Wu J, Li HW, Wang T. Hepatoid adenocarcinoma of the stomach: Thirteen case reports and review of literature. World J Clin Cases. 2020;8(6):1164-1171.
- Søreide JA, Greve OJ, Gudlaugsson E, Størset S. Hepatoid adenocarcinoma of the stomach--proper identification and treatment remain a challenge. Scand J Gastroenterol. 2016;51(6):646-53.
- Yoshizawa J, Ishizone S, Ikeyama M, Nakayama J. Gastric hepatoid adenocarcinoma resulting in a spontaneous gastric perforation: a case report and review of the literature. BMC Cancer. 2017;17:368.
- Ushiku T, Shinozaki A, Shibahara J, et al. SALL4 represents fetal gut differentiation of gastric cancer, and is diagnostically useful in distinguishing hepatoid gastric carcinoma from hepatocellular carcinoma. Am J Surg Pathol. 2010;34(4):533-40.
- Sentani K, Oue N, Sakamoto N, et al. Gene expression profiling with microarray and SAGE identifies PLUNC as a marker for hepatoid adenocarcinoma of the stomach. Mod Pathol. 2008;21(4):464-75.
Imágenes
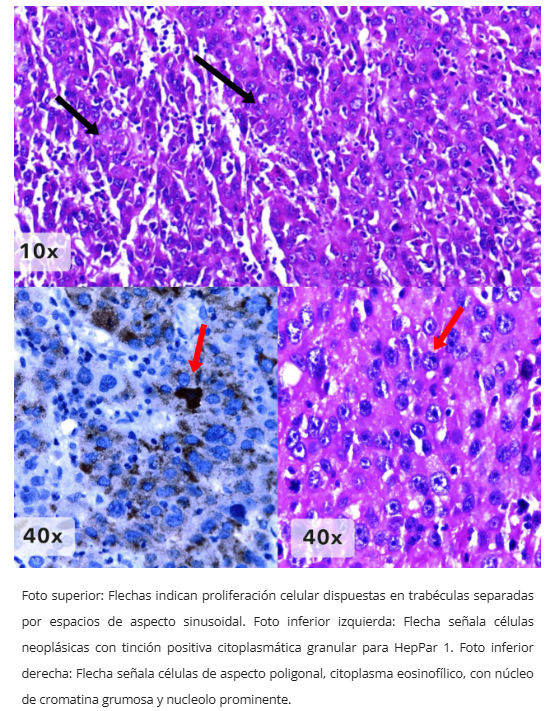
Adenocarcinoma hepatoide - Patrón trabecular
